During the holidays the Obama Health Transition Team urged people to organize discussions about health care in their homes and communities – and then to report back. Reading about these discussions – including the one that Secretary Designee Tom Daschle attended in Indiana – made me think about what things are going to be needed to make health reform actually work.
My end-of-year reflections and ruminations led me to conclude that one of the most challenging parts of health reform will be to actually get more people enrolled in whatever expanded coverage plans are developed and implemented. Enrollment barriers are not new, but they are frequently not highlighted because they may present great political and fiscal risks.
Eligible But Not Enrolled
Medicaid experts have long known that a significant number of people who are eligible for Medicaid but are not enrolled. According to a 2006 Report from the Commonwealth Fund, 62% of “uninsured children and two-thirds of uninsured, poor parents qualify for publicly funded health coverage programs but are not enrolled.” And enrollment barriers have been seen in Massachusetts as it has implemented its health insurance coverage expansion program. For example, Bill Walczak, the CEO of the Codman Square Health Center in Roxbury, (a low-income section of Boston), has stated that they have 1400 patients who are eligible for free health insurance, but they can’t get them enrolled because of paperwork barriers.
For several years, Washington DC has also had a health insurance expansion program called the Health Alliance. Unlike the Massachusetts program, there are no mandates or penalties for not enrolling. But, Bread for the City, which runs two free clinics in DC, has seen the same enrollment problems as Codman in Boston. Both Codman and Bread have staff dedicated to helping people collect and submit all the necessary paperwork, but they still have significant enrollment barriers because of clients moving, not following up on mail, chaotic lives and trouble finding the right proofs. I also suspect that literacy may be a problem for some people – since how can people respond to mail or find the right documents if they cannot read them?
Cost of Enrollment Barriers
Although the uninsured clients at Codman and Bread receive care when they show up, not having insurance makes it much more difficult for them to get needed medicines and specialty care. And of course, not having health insurance hurts people in the form of poorer health. This situation also hurts the clinics financially since they would be getting paid for this care if the patients were insured. Codman’s CEO wrote that if their 1400 uninsured patients had insurance, they would receive an additional $250,000 per year – An amount that would make a significant difference in their ability to provide care to patients. They face the quandary of whether or not to hire more people to help clients apply for free insurance, since this only makes sense if it brings in more money than it costs to hire someone.
In Massachusetts, Codman is not the only healthcare organization suffering financially from this problem. The Cambridge Health Alliance recently noted that they may have to scale back services or close one of their hospitals because of shortfalls they are seeing under the new health program – some of which is due to their not getting paid for care they provide to patients eligible for insurance.
Uninsured in Massachusetts
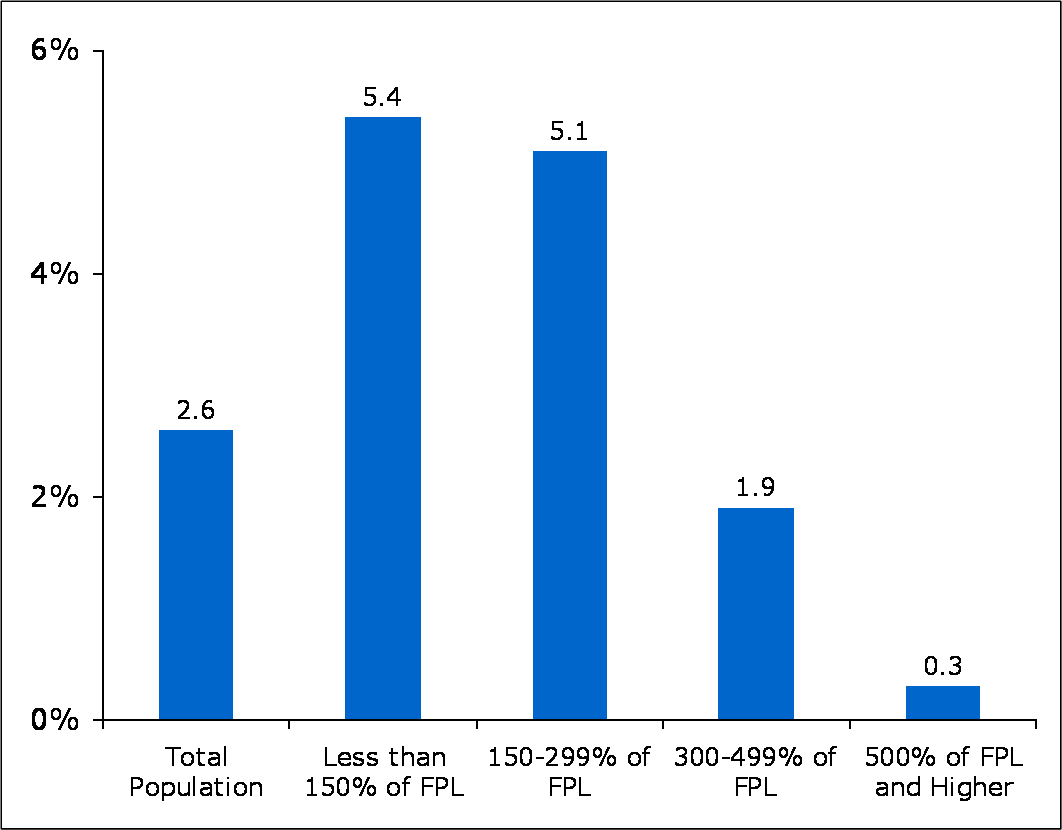
The paperwork barriers to enrollment in Medicaid, (and other free or very low cost insurance programs), also raises questions about the number of uninsured in Massachusetts. The number of people without insurance has certainly declined, with the latest report indicating that 2.6% of people don’t have insurance – a very significant decline from 7.4% in 2004 before the State’s new program began.
However, I’m curious about how well the surveys that generate these numbers are actually capturing the lack of insurance in vulnerable low-income populations – both because of the paperwork barriers and their higher rate of churning – even though the report indicates that rate of uninsurance for people below 300% of the Federal Poverty Level is more than 5% [See Chart below, and also see page 9 of Kaiser Family Foundation’s Medicaid Primer for discussion of the effects of “churning” on Medicaid enrollment.]
Solutions and Challenges
Certainly one solution would be easy and automatic enrollment. Basically, this could be as simple as the patient signing a form stating that they meet the eligibility requirements for the health insurance program. [Click here to see the Massachusetts Medicaid application]
The problem with a simple form is that it could lead to fraud – either by people who are not eligible so they can get free health insurance, or clinicians enrolling people so that they can just get bill Medicaid for services they aren’t providing. One possible solution to this fraud problem would be to require that the form be signed by both the patient (or their guardian) and the clinician (or someone in their office that they designate), BUT only clinicians that the State has pre-authorized could sign and submit the auto-enrollment forms. That way the State could limit the authorization to clinicians who already are providing care to large numbers of Medicaid patients, and thus reduce the number of organizations it would need to examine for fraud. And of course these clinicians would be responsible for attesting that these patients are believed to be eligible for the Medicaid program.
Such a system could work by having the enrollment counselor at an authorized clinic go over the eligibility criteria with the patient, and if they meet the requirements, then together they would fill out a one page form. Such a form could have the patient sign a single line which reads something like: “I believe my income is below the level required to be in the Medicaid program, as it has been explained to me by _________________ [Name of person signing below].”
And the person assisting them from the clinic would sign below stating, “I attest that, to the best of my ability and in good faith, I believe that __________________ [Name of person filling out top part of form] meets the requirements to be eligible for Medicaid. I also understand that signing this form without having discussed the actual requirements with this person or reviewing any documents they have provided or are otherwise available to me which may indicate whether or not they meet the eligibility requirements, constitutes fraud and may subject me and _________________ [Name of organization] to financial and criminal penalties – including imprisonment. In addition, if the person signing the top of this form is found to be fraudulently enrolled in Medicaid, they could also be subject to financial and criminal penalties. Thank you for assisting with this process. Your contribution to improving our healthcare system is greatly appreciated. Have a great day!”
I’m sure there are problems with such a simple form, and that other people could improve on that language. And I invite comments, edits and criticisms to this suggestion because unless we figure out how to actually enroll eligible people in free health insurance programs, then universal coverage will remain a vision outside our grasp. [Also see the Commonwealth Fund Report on how auto-enrollment might work and what Federal policies would facilitate auto-enrollment.]
Closing Observation
Anticipating that someone will suggest that other countries – like England – have figured out how to do universal enrollment and don’t seem to have the fraud I’m concerned about, I would like to note that a major operational difference between our system and England’s National Health Service is that the NHS employs the physicians and owns the hospitals, whereas Medicaid reimburses for specific clinical services. What this means in terms of financial fraud, is that the NHS has a fixed amount of money to spend each year, (like the Veterans Health System here in the US), and if they run short of money at the end of the year they have to cut back on the care they provide. Conversely, Medicaid just keeps paying the bills. So in England, if people are fraudulently enrolled in their system, they are just “stealing” resources from others in the form of preventing or delaying other people from getting the care they need. Conversely, Medicaid fraud results in Medicaid spending more money, but access to care for those who are legitimately enrolled isn’t significantly compromised because Medicaid doesn’t “run out of money” the way the NHS or the VA can.

[…] Miller has an insightful post about healthcare reform on his Health Policy and Communications Blog. We’ll be covering some of the points he raised in greater detail next week, but don’t […]
[…] Miller has an insightful post about healthcare reform on his Health Policy and Communications Blog. We’ll be covering some of the points he raised in greater detail next week, but don’t […]
Specifically, we need to invest in a new health system that can tackle the growing problem of chronic disease, which is crippling both our health care system and our economy.
Of the $2.2 trillion we pour into health care each year, a frightening 75 cents of every dollar goes towards treating patients with chronic illnesses. In Medicaid, this figure is an even more regrettable 83 cents of every dollar; in Medicare, it’s an astounding 96 cents.
Illnesses such as diabetes, heart disease, and cancer, that in many cases could have been prevented by changes in behavior or could be better managed through early detection and appropriate access to treatment, have risen dramatically over the past three decades, leaving Americans in much worse shape at earlier and earlier ages.
The rise in obesity is at the root of this increase. With younger and younger Americans suffering from overweight and obesity, the outlook is grim for finding a solution to stem rising health costs short of helping Americans transform their unhealthy behaviors.
The truth is, we can never expect to improve the affordability of health care until we face the dual crises of obesity and chronic disease. And, until we deal with cost, the chance of extending health care coverage to more Americans is grim.
Check this out:
http://blog.nj.com/njv_guest_blog/2009/03/health_care_reform_lets_do_it.html
Thanks HelicalZz – I try to connect pieces of information and provide historical perspectives to create more textured pictures of issues and situations. I think this is important in helping people understand issues, and develop solutions that can have long-term success – which is often hard when reacting to the crisis of the day or week.
Please let me know if you have any questions about any of my posts, or have suggestions for issues you’d like to see me write about.
Best Wishes, Mike
Nicely presented and well balanced. I am enjoying following your blog and find it very informational.