After spending a week in Washington DC talking to lots of people, and reading all sorts of information, I’m still not sure how to simply explain the the current state of health reform legislation – except to say that it is unfolding pretty much as expected:
- It is taking a lot longer than planned, i.e. the August deadline never seemed realistic
- There are pockets of agreement, but no solid majorities for a single bill
- The Senate and House are operating in parallel, with the Senate being more conservative and focused on issues important to rural communities
- Costs and spending are defining the framework within which all the ideas and packages are bouncing – like a 1970s video game
- And political motivations and calculations are the firmament for many – if not most – positions and actions
Politics with Elections on 12 Month Horizon
On the last point, there has recently been ample evidence. For example, the National Journal’s Insiders Poll recently asked, “On health care reform, what outcome would most benefit your party in the 2010 midterms?” The results show that both Democrats and Republicans think that the best thing for their party would be “Enacting Legislation similar to the House committee bills.” (44% of Democrats chose this option compared to 35% of Republicans, 37% of whom chose “Enact nothing”)
While there isn’t bipartisan agreement about the substance for health reform, both sides think that health reform like the House committee’s bill would be best for them politically. As a Democratic respondent stated, “A strong health care package will be popular, especially when people see that none of the predictions from the town hall crazies came true.” And from the Republican side, “With more and more Americans distrustful of government, passing the House bill would be a gift to the GOP.” The problem with the Democrat’s substantive – and probably correct – insight, is that most of the bills’ provisions won’t start until 2013 because it will take that long to create the rules and infrastructure for implementing substantive reforms. To that point, another Republican noted, “Passing the most liberal version helps Republicans: The theme for 2010 and ’12 will be, elect more Rs so we can fix this before it goes into effect.”
Other articles in the October 17th issue of National Journal also point to the highly political stakes and schisms behind health reform legislation for the Democrats:
- “Ultimately, the verdict on the efficacy of Obama’s style will depend in significant part on whether health care legislation passes, said Larry Sabato, a professor of politics at the University of Virginia. ‘Health care could be his hammer – if he gets it, he will have proven that his style works, that you don’t have to be an in-your-face LBJ type to get significant health reform. But if it falls apart or he gets a tiny piece of it, then there will be criticism that he is ineffective and not tough enough.'” (From “Is Obama Tough Enough?”)
- “Although health care is becoming ground zero in the economic and values conflicts that loom within the Democratic majority, a host of other issues also have the potential to undermine party solidarity.” (From “Democratic Fault Lines Open Up.”)
To negate the Republicans’ ability to leverage people’s fear of change as they pick apart proposed rules and regulations – while also proposing legislative changes and repeals – some Democrats have called for more of the benefits to start earlier, i.e. before 2013. However, starting some benefits earlier would increase the 10 year costs of the new law, and – in contrast to expanding existing programs like Medicaid – many provisions would require new programs and rules. Both of these factors make earlier implementation both practically and politically very challenging.
Despite these realities, and the political intricacies of the US Senate, Majority Leader Reid has taken control of melding the Finance and HELP Committees’ bills and is apparently steering it in a direction to address his reelection concerns in Nevada – at least according to the Washington Post’s Dana Milbank.
Another political complication for moving health reform legislation forward this week – as Speaker Pelosi has indicated – is Tuesday’s elections across the country. Normally moving things forward in a speedy fashion would be good, but asking Members to vote on something so potentially politically contentious right after local elections in their home areas may make them hyper-sensitive about their reelection concerns.
Coverage Beats Cost Containment Like Rock Covers Paper
Within the twin goals of having health reform legislation cost less than $1,000.000.000,000.00 over ten years and not adding to the Federal deficit, legislation has evolved to focus on expanding coverage while drifting away from significant changes to healthcare delivery that would control long-term spending. This has occurred for two reasons: Spending money on coverage expansion is relatively easy, while changing the operations of the delivery system is much harder, and actually requires more than just financial incentives.
The extent of this shift is described in the recent analysis of HR 3200, (as passed by the Ways and Means Committee), conducted by the Actuaries Office at the Centers for Medicare and Medicaid Services. Although the Congressional Budget Office is the arbiter of the official cost estimates for legislation, they focus on federal costs, while the CMS Actuary analyzed the effects of the legislation for total healthcare spending, as well as expansion of insurance coverage. Looking at the numbers in their report for the years 2013 and 2019 are very informative:
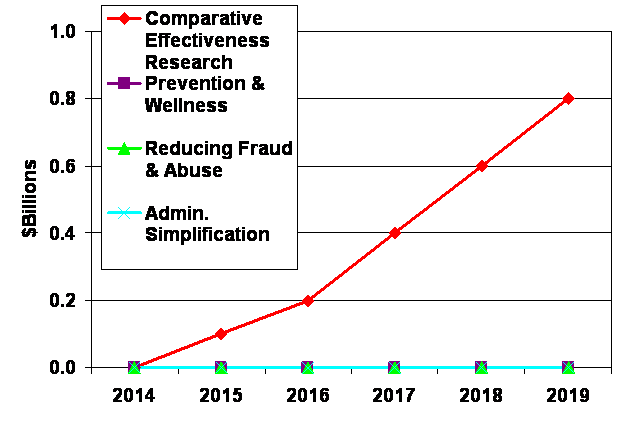
First, the actuaries estimate that the four provisions intended to reduce healthcare spending would have minimal impact, with only comparative effectiveness research reducing spending by a few hundred million of dollars out of total spending estimated to be over $4.6 Trillion in 2019:
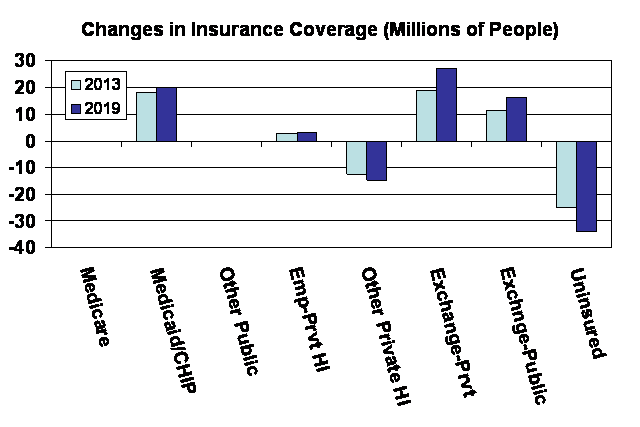
Second, the actuaries estimate that the legislation would increase insurance coverage through Medicaid/CHIP and via the Exchange, while having no effect on Medicare and little effect on employer provided health insurance. Overall, the legislation is estimated to reduce the number of uninsured by 33.9 million in 2019, leaving 23.0 million uninsured – including unauthorized immigrants, which others have estimated to currently total ~6-7 million:
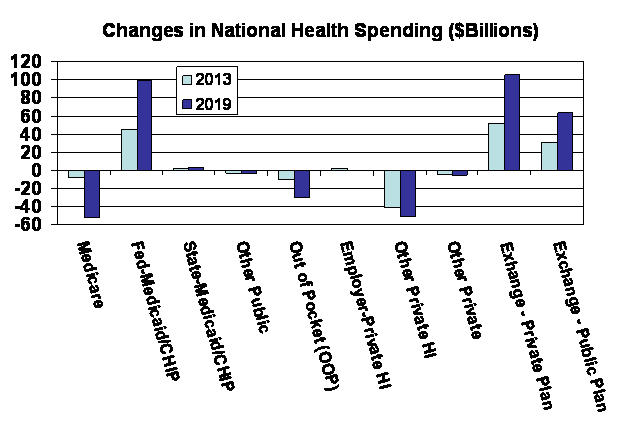
Third, the actuaries estimate that the legislation would reduce spending on Medicare, and private out-of-pocket and direct insurance purchases, while increasing spending for Medicaid/CHIP coverage, and for insurance acquired through the Exchange – both private insurance and the proposed public plan option:
Bottom Line – Start Making Sense
It is looking more likely that a bill will be enacted before the end of the year – but that outcome is far from certain. If passage of legislation doesn’t occur by the end of December, there are three other possible outcomes:
- The bill – and various amendments – could be brought to the floor to allow Members to go on record about health reform overall and various specific issues. (This presumes that a bill isn’t brought to the floor with the expectation of passage, but fails.)
- Negotiations are carried over into 2010 because the Democratic leadership doesn’t have the votes to pass a bill in December.
- With the outlook for getting enough votes for passage looking bleaker as the 2010 elections loom closer, the Democratic leadership could decide to shelve major health reform legislation, cobble together a bill of Medicare and related changes that are needed, and pass that bill at the end of December.
The first and third outcomes would bring closure (if not cloture) to the process and create space for other issues requiring Presidential and Congressional attention. The second route would prolong the debate and maintain the possibility of passage – but with decreasing likelihood.
In addition, as a major health reform legislation is being debated in Congress, it is very unlikely that the Administration will nominate an Administrator or Deputy Administrator for CMS. This makes sense because presenting a nominee would divert attention in the Senate, and whoever is nominated would face an armada sized barrage of questions about ever large and minute issue in the pending legislative proposals. However, it also leaves CMS without its full compliment of political leaders, which could be a problem in 2010 whether they are tasked with implementing large parts of a new health reform law, or more focused changes to Medicare and Medicaid.
So will healthcare reform start making sense to the average voter, or will the whole issue blow up for Democrats in the 2010 election – either through failure to pass anything or by overreaching and fueling the wild-eyed fires in the red and purple pockets on political strategists maps? The answers to these and other questions about the policies and politics of health reform will come sooner or later – and certainly by November 2010.
p.s. What the Talking Heads Said in “Stop Making Sense”
There are some interesting insights and parallels about the current health reform situation from the Talking Heads’ 1984 film “Stop Making Sense.” In particular, there seems to be some prescient message in the titles of a few of their songs included in the movie (with my annotations):
- Psycho Killer – (Rabidly opposing health reform based on disparaging mischaracterizations?)
- Slippery People – (No comment necessary)
- Burning Down the House – (The goal of the Republicans? Or what the Democrats could achieve by overreaching or mishandling health reform?)
- Making Flippy Floppy – (What is a public option and why?)
- Swamp – (Will health reform get mired in a swamp?)
- Once in a Lifetime – (What many health reform advocates think this is?)
- Crosseyed and Painless – (How many people working on health reform feel right now?)
