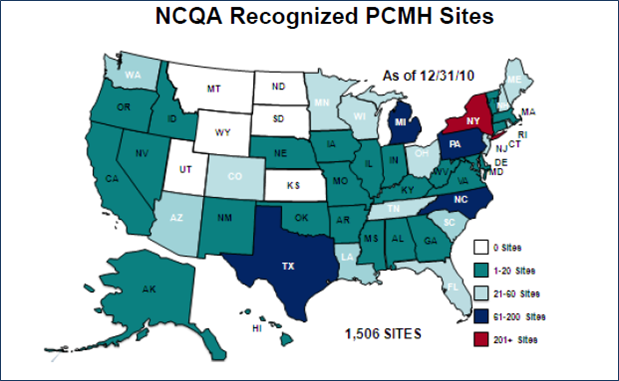
Patient-Centered Medical Homes (PCMH) are continuing to be a bigger and broader part of the real-world discussions about health reform and transformation in the US. According to the the National Committee for Quality Assurance (NCQA) at the end of 2010 there were 7,676 clinicians in 1,506 recognized PCMH practices in the US. This information was released last week by NCQA with their updated 2011 PCMH Standards.
Another marker of medical homes’ increasing pervasiveness is the blurb – “Home sweet medical home” – in the March 2011 issue of Consumer Reports magazine that starts with, “If you haven’t already heard the term ‘patient-centered medical home,’ chances are you will soon.”
Consumer Reports – “Home Sweet Medical Home”
The Consumer Reports blurb is part of an article about what primary care physicians wish their patients knew. Interestingly this longish blurb notes that any practice can be more patient-centric without being officially certified, and it lists the important features patients should look for:
- Can you get an urgent appointment within 24 hours?
- Can you reach somebody in the practice by phone at night or on weekends?
- Can you get test results quickly via e-mail or telephone, or on-line?
- If you have a chronic condition, is there a system for tracking how you’re doing?
- Does the practice include non-MD staff members such as nutritionists or nurse practitioners to help you manage your medications or chronic conditions?
- Does your primary-care doctor keep track of your treatment by specialists?
NCQA’s 2011 PCMH Recognition Standards, Elements, and Factors
The 2011 PCMH Standards NCQA released last week are much more detailed about what a primary care practice should look like to provide high quality primary care – and they are a logical evolution from their 2008 Standards. Specifically they:
- Reduce the number of Standards from 9 to 6 – which should make them easier to understand and implement.
- The 6 Standards have multiple Elements. And each Element has various Factors that contribute to the scoring for that Element.
- Integrate newer health IT standards and requirements.
- NCQA provides a cross-walk between the Elements and the corresponding Federal Meaningful Use requirements for health IT that enable clinicians to receive higher Medicare and Medicaid reimbursements.
- Include a patient survey, which will be available in 2012.
- The optional survey will provide more patient-centric feedback about people’s experiences and enable practices to score extra points towards the recognition Tiers.
NCQA also continues to have three Tiers of possible recognition – with Tier 3 being the highest.The new NCQA standards also continue to have “Must-Pass” Elements (in bold/italics below) for the 6 Standards. And practices must score at at least 50% on all those Elements to receive any recognition Tier.
Standard 1: Enhance Access and Continuity
Access During Office Hours, e.g., same day appointments and telephone or email communicationsStandard 2: Identify and Manage Patient Populations
Use Data for Population Management, e.g., using medical record data to remind patients about getting evidence-based care for specific preventive services and treatments for chronic conditionsStandard 3: Plan and Manage Care
Care Management, e.g., individually written care plans and addressing barriers to patients achieving their treatment goalsStandard 4: Provide Self-Care and Community Support
Support Self-Care Process, e.g., providing educational resources and tools to enable patients to improve their self-care and healthy lifestyles/behaviorsStandard 5: Track and Coordinate Care
Referral Tracking and Follow-Up, e.g., coordinating and following-up on referrals to specialists, including testing done by specialists and their recommended treatmentsStandard 6: Measure and Improve Performance
Implement Continuous Quality Improvement, e.g., setting goals and acting to improve care for patients with chronic conditions, (such as diabetes, heart disease and depression), and preventive services, (such as immunizations, and cancer and osteoporosis screening)
It is also worth noting that among the various Factors that make up the Elements, NCQA designate some as “Critical Factors,” i.e., they are required for any scoring on that Element. And two of these Critical Factors are for Must-Pass Elements:
- “Providing same-day appointments”
- “Develops and documents self-management plans and goals in collaboration with at least 50% of patients/families”
Thus, to achieve any level of recognition as a PCMH from NCQA, practices must have these two capabilities.
Conclusions:
While it may be coincidental that Consumer Reports lists 6 criteria for patients to consider in evaluating primary care practices for their “medical homeness,” and NCQA has 6 Must-Pass Elements, the two lists do parallel each other.
NCQA and Consumer Reports are targeting different groups of stakeholders – which is appropriate. NCQA’s requirements enable practices and providers to become recognized, while also informing payers and regulators so they can determine how to utilize a practice’s recognition in their policies and practices – including reimbursement levels.
Similarly, Consumer Reports is seeking to educate consumers, (a.k.a. patients and families). What is reassuring is that Consumers Reports doesn’t try to compare medical homes or clinics using its normal format of tables of numbers and those great red and black circle symbols. That type of evaluation works well for commodities like TVs, but medical care is a process not a product, and it needs to be individualized for the patient – so what is a good medical home for one person may not be as appropriate for another. (Atul Gawande’s recent New Yorker article “Hot Spotter” includes some examples of how cultural appropriateness can be a determining factor for the success of care for severely ill people.)
NCQA’s standards focus on structures and processes, and thus are not the beginning and end of what is needed for a successful patient-centered medical home. But certainly rigorous structural and process standards, combined with consumer education – along with other contributing drivers like cultural change motivators and incentives for achieving better outcomes – should lead to better quality, value, and efficiency in our health care system.
Let me know what you think about Medical Homes.
[Full Disclosure: I was given the Consumer Reports magazine by a friend who bought it because it has an article about TVs – and now I have to help her go buy a TV.]
