If all arrows in Washington pointed to the same spot for solving the healthcare and Federal spending problems could the politicians, pundits and policy people agree? Or would it take some new and powerful force to shine a spotlight and focus the collective vision on this solution, and what would that force be?
These are the two questions I’ve been asking myself as the battle over Federal spending has become near white-hot, and as it has become increasingly clearer that long-term Federal solvency and deficit reduction will require addressing the growth in healthcare spending – particularly Medicare.
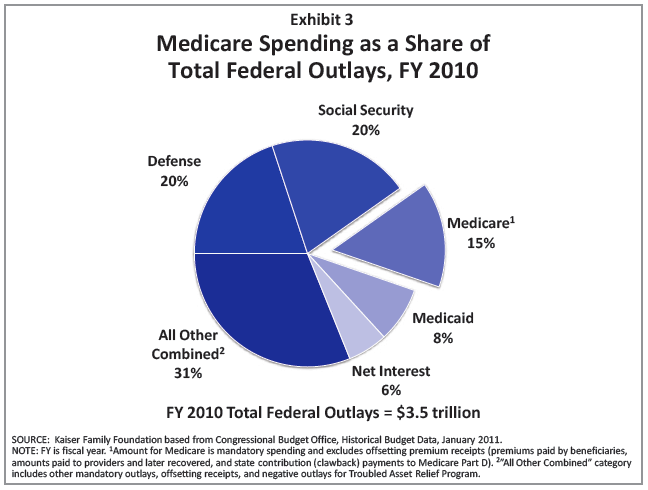 [Source: Kaiser Family Foundation “Medicare Spending and Financing,” February 2011]
[Source: Kaiser Family Foundation “Medicare Spending and Financing,” February 2011]
To summarize the highlights of this situation:
- Cutting non-defense discretionary Federal spending can’t produce the reductions needed to significantly impact the deficit – contrary to the general misunderstanding about how the Federal budget is spent. (See this recent Washington Post article, and the bullet below from an associated poll.)
- “There are widespread misperceptions about the state of the federal budget. A majority of voters incorrectly believes the federal government spends more on defense/foreign aid than it does on Medicare and Social Security (63%). Also, a similar majority (60%) incorrectly believes problems with the federal budget can be fixed by just eliminating waste, fraud and abuse. Voters do not casually agree with these untruths- at least 40% strongly agree. Further, less than half (44%) believe Medicare and Social Security costs are a major source of problems for the federal budget (49% disagree).”
- Medicaid spending is high but counter-cyclical, so improvements in the economy and employment will reduce those costs by cutting the number of people using the program
- Social Security is a straight numbers issue – while the Baby Boomers are increasing the program’s numbers, the per person cost growth is close to CPI
- Medicare is not counter-cyclical, its growth is a combination of the Baby Boomer influx and the per person growth rate, which is projected to be about 7%. The result is that since Medicare accounts for about 15% of total Federal spending, the Medicare program is the keystone to solving the Federal fiscal puzzle
Solving the Medicare Puzzle
Wouldn’t it be great if there were a way to reduce Medicare long-term spending, and one that most politicians and policy people agreed was the right solution? Fortunately there is. And it’s already in Federal law: It’s a concept that many Democrats and Republicans have repeatedly endorsed because it increases local control and decision-making, while shifting incentives from quantity of services to quality of care. This new model is called Accountable Care Organizations (ACOs), and it was included in the new health reform law, (a.k.a. Patient Protection and Affordable Care Act, or “Obamacare”). This short provision in the law adds ACOs as a fundamental change to Medicare, (i.e., not just a pilot or a demonstration), and it enables Medicare to pay ACOs in any way that both Medicare and the healthcare provider (or delivery system) agree to. Further, it encourages Medicare to work with private payers to enhance the motivations for creating successful ACOs. [See 1899(i)(3) and 1899(j) of Title XVIII of the Social Security Act (42 U.S.C. 1395) as added by Public Laws 111-148 & 111-152.]
So why isn’t there a collective multi-partisan and multi-stakeholder rally of support for ACOs?
- Making healthcare delivery systems and providers into effective ACOs won’t happen quickly – it will require a stepwise transition. (However, many, many hospitals, health systems, group practices and others are gearing up for the transition – which will likely involve bundled payments and focused bonuses for achieving desired outcomes – but the roads to becoming a full ACO will be varied and lead to many different successful structures.)
- The proposed rules for the ACO provisions of the health reform law haven’t been issued yet, so there is still significant uncertainty about how Medicare will implement their new authority.
- Political philosophy against government programs – particularly on the national level – is now a very strong force focused on repealing “Obamacare” like college students during spring break fixated on a blinking “Free Beer” sign.
- The ACO provisions lack the specific payment formulas or dollar amounts that fiscal forecasters desire for building models and developing multi-year estimates. As a result, the savings projections, (a.k.a. scoring), have estimated only very modest reductions in Medicare spending since there is significant uncertainty about how ACOs will develop and evolve.
Solutions
Here’s why those savings projections are too conservative, and what can be done to swing the political tide the other way:
- Hospitals, healthcare systems, other providers, and other organizations are already preparing to become ACOs. That is, rapid movement towards ACOs is happening across the country, and it needs Medicare to be a positive – and maybe even aggressive – supporter. This private sector movement is similar to the reaction health providers and payers had to the potential national health reform legislation in 1993-95 – (see chart below) – but this time the reform is actually in law, and the private sector responses are much broader and intense…. From what I am seeing, this activity is about 10 times greater in terms of resources being committed, and plans being developed and implemented.
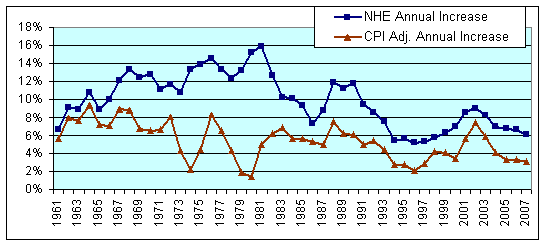
[National Health Expenditure Increases: Actual and Adjusted for CPI]
- The other “solutions” to reducing Medicare spending are the typical “cuts” in payments to hospitals and doctors, or reducing benefits to seniors…. But for either of those to significantly reduce long-term spending would require politically and socially untenable changes to Medicare. In addition, these changes would involve much greater Federal government intrusion in actual care delivery decisions than would effectively implementing the ACO provisions of the ACA.
- For Americans to be receiving UnAccountable Care as the norm is no longer acceptable – just as driving cars without seat belts or dumping raw sewage into rivers is also not acceptable today, even though it was the norm in the past. Just as the standards of care for medical practice change, so should the overall structure of care delivery. For example, high blood pressure in the elderly used to be accepted and not treated because the thinking was that the high pressure was a good thing and needed to push blood through hardened arteries. That idea is no longer accepted, and not treating hypertension today would be UnAcceptable care.
- There needs to be a public groundswell for “Accountable Care Now.” This can be true grassroots support, grass-tops advocacy from opinion leaders, and even “astro-turf” campaigns from national advocacy organizations and companies. The end result needs to be getting public opinion and voices to be coherent and loud for change. What matters is that the chorus for “Accountable Care Now” sound something like:
What Do We Want?
Accountable Care!
When Do We Want It?
Now!
Bottom Line
If Medicare beneficiaries, organizations paying for healthcare, (including Medicare and Medicaid programs), and everyone else – including leading healthcare professionals – start a drum-beat for “Accountable Care Now,” it will become UnAcceptable to be delivering or paying for UnAccountable Care. And elected officials across the spectrum, pundits, and policy leaders will have to – and want to – start looking under the Accountable Care spotlight and put their efforts toward making Accountable Care a reality Now – or at least ASAP.

[…] have previously written about Accountable Care, (and how it is fundamental for successful health reform), and with the unveiling of the menu from […]