Healthcare innovation is an extremely hot topic right now, ranging from the new Center for Medicare and Medicaid Innovation, FDA’s approach to approving therapies and devices, an entire issue of Health Affairs, and of course patient-centered medical homes and Accountable Care Organizations [Patient-centered medical homes are also known as Advanced Primary Care Model practices, and ACOs are a combination of delivery and reimbursement innovations.]
I’ve been working for many years to create value for patients and society by speeding adoption of these types of innovations by clinicians, other providers, patients, payers, regulators, communities, etc., and have found that healthcare innovations have at least three things in common:
- Healthcare innovations occur in steps, with each advance building on the shoulders of what came before
- These stepwise advances also produce indirect benefits that can be greater than the innovation’s direct effects
- Adoption of innovations doesn’t just “happen.” Strategic planning can improve the speed and breadth of adoption – leading to greater value for patients and society
1. Axes of Innovation – Primary, Secondary and Tertiary Benefits
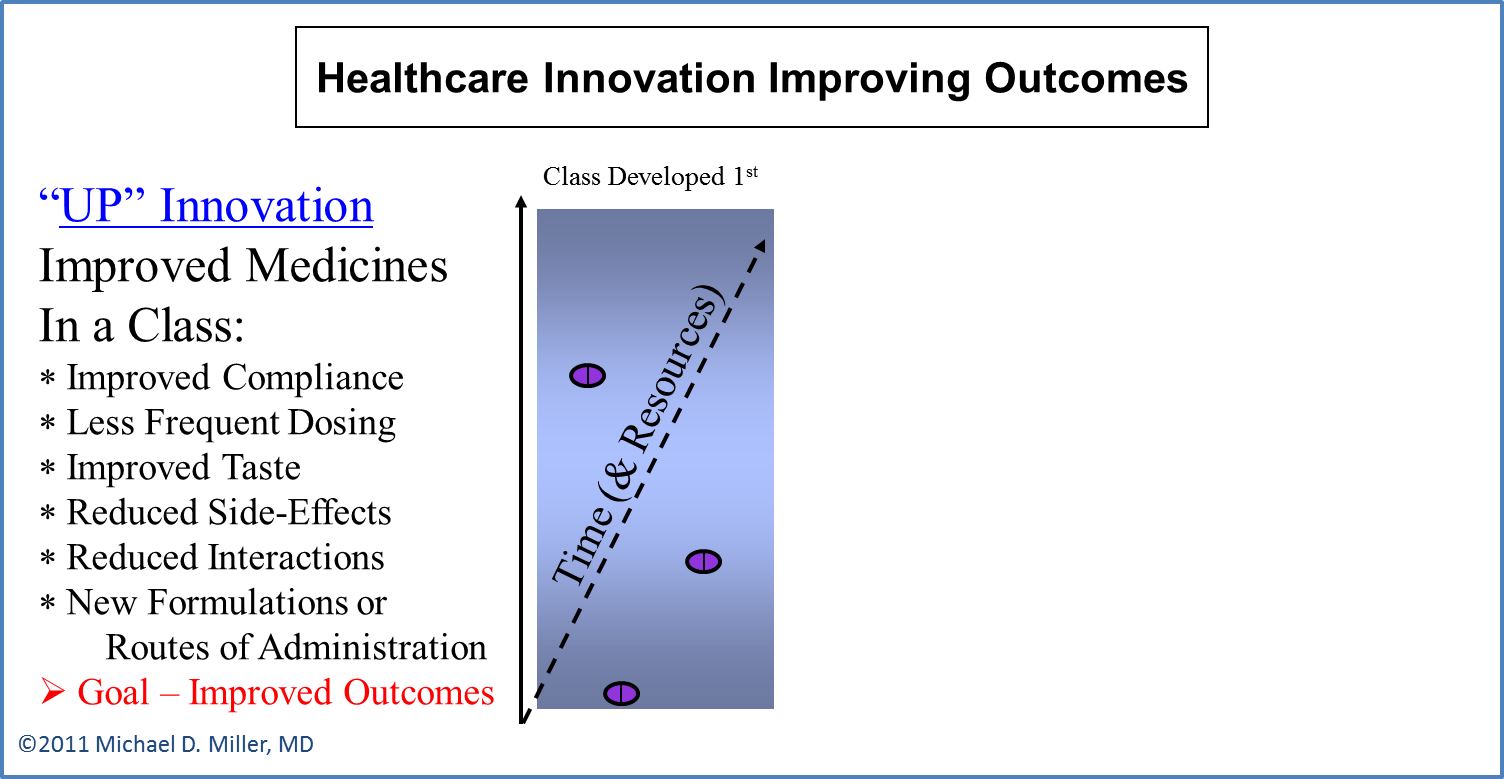
Every healthcare innovation can have multiple benefits to patients and society – often for different conditions. I call this cascade of different benefits UP, OVER, and OUT Innovations. (The text and diagrams below illustrate this biopharmacueticals.)
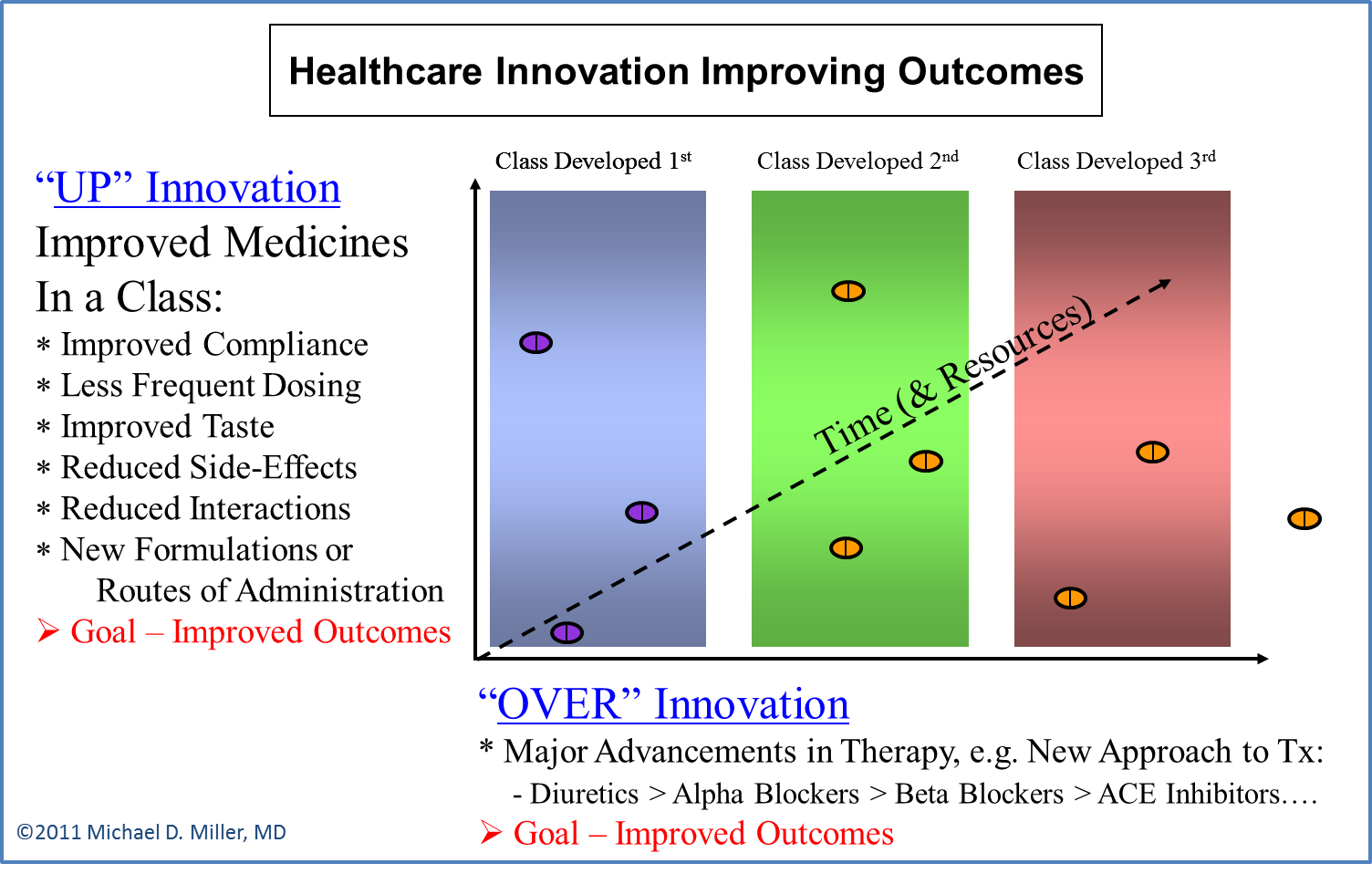
UP Innovation: UP Innovations occurs when subsequent medicines in a class, (e.g. Beta Blockers for high blood pressure), have characteristics, (such as once-a-day dosing, and less side-effects or drug-drug interactions), that permits more patients to use the medicine correctly, and thus produce better outcomes.
OVER Innovation: OVER Innovations occur when medicines are discovered that treat the same disease through different mechanisms of action, such as Beta Blockers and ACE Inhibitors to treat high blood pressure.
OVER Innovation also occurs across industries and platforms when devices and other therapies are developed that compete with biopharmaceuticals – and vice versa. This occurred for erectile dysfunction (ED), when devices, (both the vacuum pump made famous by Austin Powers and implanted prosthetics), and an injectable medicine, presented different treatment options. These therapies all had certain characteristics that caused patients to not use them very widely – which provided the clinical opportunity for the oral medicine sildenafil (Viagra®) – and then the other subsequent UP Innovators in the PDE5 Inhibitor class of pills.
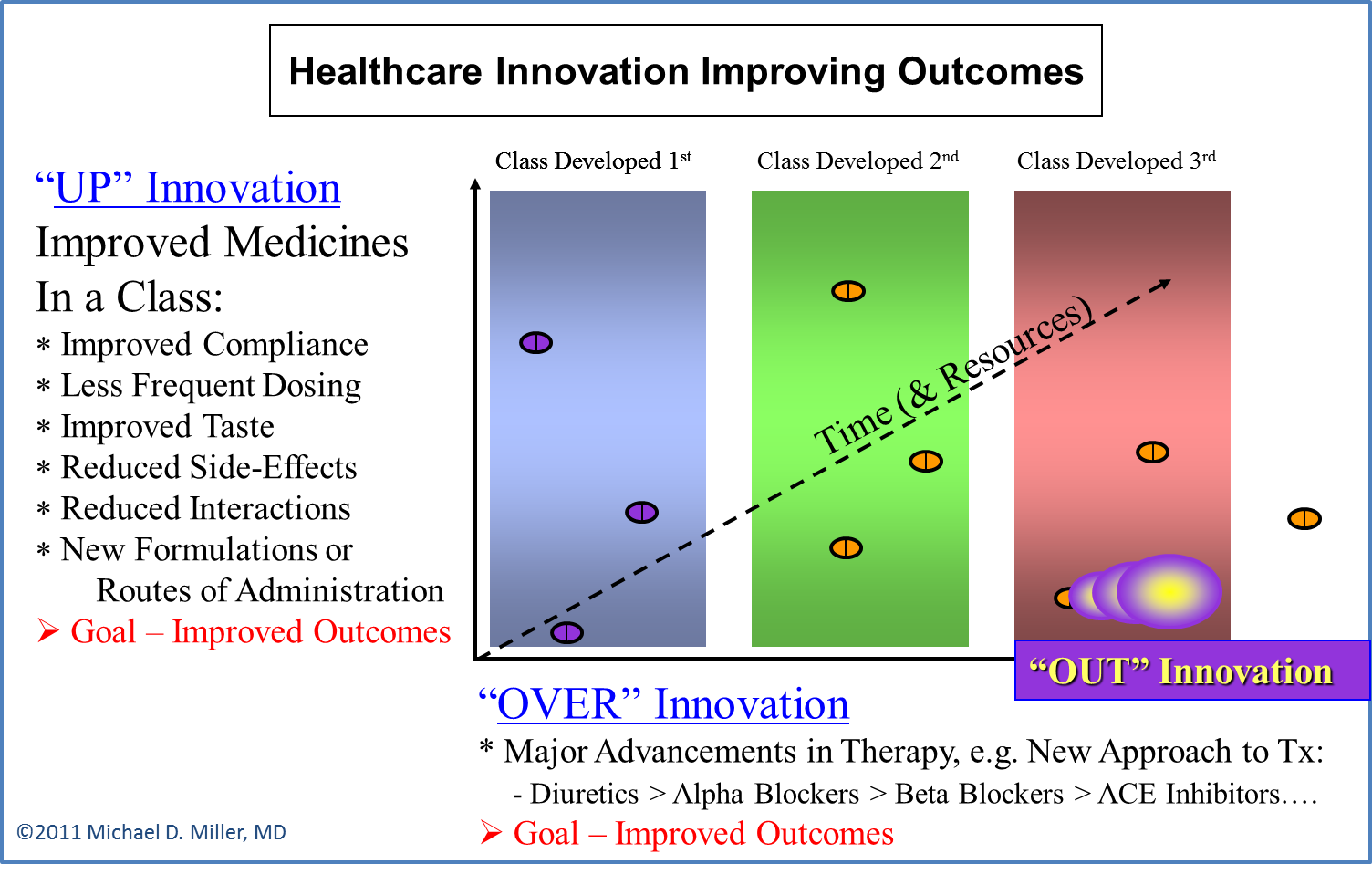
OUT Innovation: OUT Innovation involves the use of an existing therapy for completely new diseases or conditions. Sildenafil to treat early-stage pulmonary arterial hypertension is an example of this type of innovation. (You didn’t think I used Viagra® in the previous example just to be salacious did you?). Similarly, many medicines to treat cancer were originally approved for a specific type of tumor and then used for other cancers, or even for non-malignant conditions. (Oncology and immune disorders such as rheumatoid arthritis are also clinical areas where small molecules and biologics compete as UP and OVER Innovations.)
2. Innovations Enable Many Types of Benefits
Another way to view the benefits innovations have for patients and society is to examine how the adoption of an innovation produces indirect changes in care delivery and reimbursements – some of which can be more significant than the innovation’s original change:
- New treatments can change how care is delivered, e.g., stents, (originally developed for urology), expanded the treatment options for clogged heart arteries from surgery to include outpatient invasive radiology procedures.
- Payment systems for specific illnesses have influenced the development of therapeutic options and care delivery infrastructure, e.g. low reimbursements for chemical dependency present barriers to R&D in that area, while high profit opportunities for cardiac rehab and obstetrics have prompted health systems to build new facilities for those conditions.
Health information technology (HIT) is a great example of a class of innovations with broad enabling effects. At a fundamental level, having clinical information in electronic forms improves the efficiency of storage and transmission, and thus reduces the time (and costs) for copying, billing and looking for records, as well as minimizing the need for repeat tests etc. (This was one of the benefits of HIT that President Obama cited in a State of the Union address.) However, the value of electronic medical records (EMRs) and related HIT applications for patients and society is even greater than these direct benefits because it enables activities such as:
- Tracking mechanisms to make sure patients are receiving recommended treatments and preventions
- Automatic checking for drug-drug interactions and patient allergies
- Easy access to recommended diagnostic and therapeutic protocols based upon the individual patient’s condition
- Systems to evaluate the overall progress of physicians and practices in meeting recommended standards of care, such as A1C levels and blood pressure for people with diabetes. (See here for an example of a web-site reporting this type of information.)
- Research across a community to identify trends in care patterns and illnesses to better allocate resources for quality improvement and public health initiatives.
Furthermore, advanced HIT applications can enable overall healthcare integration and care coordination via care teams – which leads to better care for individual patients and more rapid adoption of evidence-based practices that improve quality and efficiency. These effects are particularly evident with telemedicine, which can literally force different clinicians and caregivers to work together as a team because they are connected via a sharing technology that clearly demarcates their roles, i.e. monitor/manager and actual deliverers of care. (The draft report Telemedicine’s use in Intensive Care Units describes an example of this in more detail.)
Payment Innovation Enables Quality Improvement
Another example of how one innovation can produce significant secondary benefits is payment innovation’s potential to turbo-charge quality improvement programs: The fee-for-service payment system in the United States often penalizes clinicians and health delivery systems for providing the best quality care. For example, if a hospital/health system provides coordinators (such as social workers) to patients being discharged from the hospital or emergency room to make sure they get proper follow-up care, they are less likely to “bounce back” to the ER or hospital. (This is good quality coordinated care.) However, in many cases the hospital or health system doesn’t get paid for those follow-up outpatient services, and by preventing repeat inpatient and ER visits it also loses potential revenues.
Payment innovations – if properly structured and implemented – can reverse these types of incentives and lead to less overall spending, as well as broader and more rapid adoption of quality improving practices. Such payment innovations could involve bundling reimbursements around an episode of care, (or treatment of a condition for a month or year), or across broader care teams such as the hospital, outpatient physicians, home health and rehabilitation. And, just to come full-circle, by creating the capabilities for monitoring quality and spending, HIT systems enable accountability of health systems, providers and clinicians – as well as payers, patients, and public health officials. That is, such monitoring can ensure that the care delivered in response to the payment innovations are quality and efficiency based, and don’t lead to rationing and budget cuts disconnected from overall costs or quality.
3. Change Adoption – Faster, Sooner, Better
A third important aspect of innovation is that it needs to be adopted in order to produce value. (Duh.) While there has been a lot written about adoption of innovation, it is particularly challenging in the healthcare environment where the “product” is a service delivered very directly (and often intimately) from person-to-person. That is, healthcare is largely a service industry, and thus getting clinicians and patients to adopt an innovation is much more complicated than convincing people to purchase the latest tablet computer, or even to use self-scanners at grocery and drug stores.
Below is a simple graph illustrating the importance of strategies and steps to promote the adoption of innovation in healthcare. The two diverging lines shows why planning for and investing in change adoption are very important for actually changing clinician and patient behaviors.
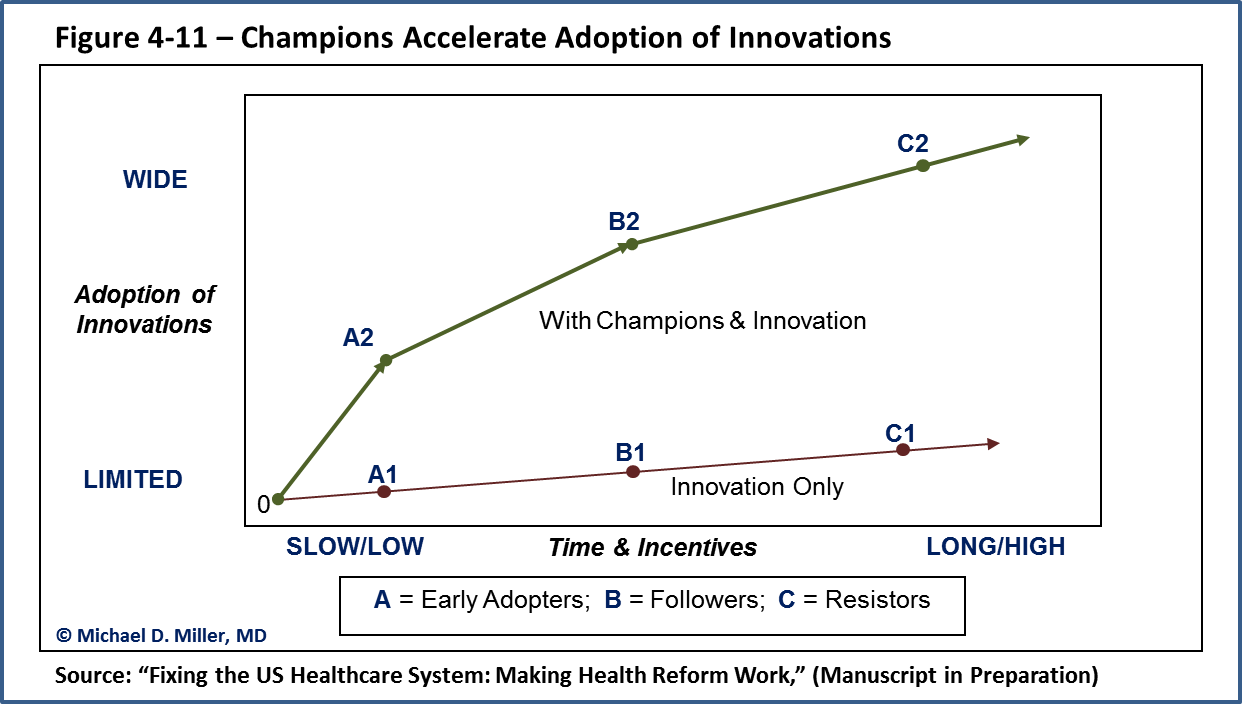
The specific strategy illustrated in this figure involves creating and supporting champions for the innovation. These “change agents” are people who can connect to the targeted users and demonstrate the value of the innovation in a real-world way. The two curves in the diagram show the difference between the adoption of innovations when they are just released into the wilds of the healthcare system, (lower line), and when they are actively promoted with an adoption strategy. Specifically, the adoption of an innovation would proceed without these champions for change from point 0 to A1, B1 and C1, etc. But with champions, the path can proceed along the upper line from point 0 to A2, B2, and C2, etc. (The value of investing in the champions and change adoption strategies can be calculated by the vertical distance between the points A1 and A2, B1 and B2, etc.)
Value to Whom
How the value of an innovation is demonstrated to potential adopters depends upon the specific innovation, but generally it requires the champion presenting the information to be a peer-leader, to communicate the relevance of the innovation to the individual, and to demonstrate how the innovation will create a better situation for the individual adopting it.
This last point is crucial for adoption of healthcare innovations – such as the post-discharge care coordinators mentioned above – because many innovations may benefit patients or society, but to the individual adopting the innovation the costs would be greater than the benefits. This is what I call the “Value to Whom?” analysis since it highlights that an ROI calculation about an innovation that aggregates the costs and benefits for all stakeholder may be misleading if the costs are borne mostly by one stakeholder while the benefits are received mostly by another, i.e. their is a value mismatch across stakeholders.
Similarly, many innovations will present differential benefits (and ROIs) for different types of patients based on their clinical states. For example, while the team-based care embodied in patient-centered medical homes is good for all patients, it clearly should be of the greatest benefits to people with the most complicated and chronic conditions.
SUMMARY – The Healthcare System’s Bones are Connected Like a Skeleton (or Gears in a Machine)
- Innovations Build on Each Other: Innovations are developed based upon new knowledge, they build upon the existing “standard of care.” But the adoption of innovative treatments, delivery methods, and payment models is not a unwavering process. Rather, the breadth and depth of adoption is greatly influenced by factors intrinsic to the innovation, the clinical/economic environment in which is will be adopted, and how effectively it is presented to those who need to adopt it, i.e. clinicians, patients, payers, regulators, etc…..
- Innovations Need to Fit Into the Existing System In Order to Change It: Innovations don’t occur in isolation. Innovations are adopted into highly connected healthcare delivery and financing systems.

- Innovations Have Many Connected Benefits: Important innovations not only have direct benefits, but also create changes in the fundamental delivery of care – both by individual clinicians and within the overall structure of the healthcare delivery system. HIT and payment innovations can produce of these types of “game changing” benefits.
- Adoption of Innovations are Connected to Reimbursements: The adoption curves for innovations are tied to financial incentives. This is part of the “Value to Whom” reality. Therefore, reimbursement amounts and policies can create incentives or barriers to the development and adoption of innovations – and thus greatly influence the benefits patients and society eventually derive from any innovation.
- Innovations are Necessary for Progress: Without innovations – and without the adoption of innovations – healthcare delivery will not improve, and progress towards better quality care and lowered costs, (a.k.a. bending the cost curve), will be very slow and overwhelmed by the wave of Baby Boomers soon to hit our healthcare systems.

Appreciate Dr. Miller’s contribution here.
I’m all for more efficient health care and support innovations.
Considering innovations should also deal with the question if a new approach will
serve the patient. It also should not be too complicated.
Some important information about Health care innovation is given. It is very useful and interesting to know about it. Good article.
Wonderful information about Healthcare innovation is given in a detailed manner. Nice article.