A few years ago I was asked to write a Forward for a book about the transformation of healthcare in the US. I recently came across what I’d written about the rapidly changing US healthcare system and the challenges of controlling the growth in spending. I’m sharing it below (in the original Courier font) because what I’d written still is applicable for today’s situation, and particularly the summary sentence: “If today’s leaders — both health professionals and politicians — make wise decisions to support and foster integration of the delivery system and administrative standardization, while guaranteeing universal coverage, we will have a strong health system to support a strong nation.”…
Healthcare Prevention – Value, Savings and Strategies
Prevention is often portrayed as either the savior or the step-child for reforming, transforming, or saving the US healthcare system. How prevention would specifically benefit people and society is presented in various ways to make these points:
US Doing Worse in Prevention Activities
The Commonwealth Fund recently released a study showing the US is doing poorly in reducing deaths from preventable causes. (Variations in Amendable Mortality – Trends in 16 High-Income Nations.)
While this study isn’t a definitive prescription for systemic changes, it illustrates the performance deficiencies of the US healthcare system – and is consistent with other reports looking at related metrics.…
Selling Healthcare Changes – Loss Aversion & Adoption of Innovations
Healthcare issues ranging from national health reform to stem cell research have become a major force in political rhetoric – often overwhelming substantive information. This creates challenges for individuals and organizations seeking to achieve positive changes as their communications are swamped by election-driven messaging.
Creating and implementing successful communications programs in this turbulent environment is easier when the principles of “loss aversion” and the factors affecting the adoption of innovations are used constructively.
Loss Aversion & Campaign Messages: Swinging Votes Not Actions
Campaign communications – particularly negative messages – are very effective because they use loss aversion principles to leverage people’s reluctance to embrace change.…
Fixing or Fracturing Medicare?
Reducing Medicare spending has been one of the focal points in the debt ceiling negotiations, and it was reported that the President is considering throwing the idea of raising the eligibility age for Medicare into the pot as part of a stone soup recipe that might get enough Congressional Ds and Rs to swallow the end product.
Increasing Medicare’s Eligibility Age is Bad Policy and Worse Politics
While increasing Medicare’s eligibility age to reduce spending makes simple arithmetic sense using the formula Spending = Number of People x Spending per Person, like almost everything in healthcare, what is simple is often 30 degrees wrong.…
Patient-Centered Care? Or Not?
The term “patient-centered care” has increasingly been used to describe healthcare structures that deliver better quality care – as well as often doing so with lower costs. And today there was a news story about how some medical schools are assessing applicants’ interpersonal skills, something that is fundamental for being a patient-centric clinician.
While there are have been numerous articles demonstrating the value of patient-centered care and concluding that it is better and should be promoted – including those looking at the ill named “Patient-Centered Medical Homes” – I’ve found myself pondering the following questions:
“What type of care have clinicians been providing if it hasn’t been patient-centered?…
Cultivating Health Reform and Transformation
Listening to various speakers at a two-day HIT/Delivery System Transformation Summit last week reinforced my thinking about the concept that reforming (or transforming) the US healthcare system is more like farming than business management.

Transforming healthcare is like farming because it involves cultivating collaborations and coordination among independent people, organizations, and stakeholders who all have varied interests and reporting/governance structures. In this way, “managing” or “leading” health transformation is like growing plants – the soil needs to be prepared, the plants (or seeds) need to be planted, and then they need to be watered, fertilized, weeded, pruned, etc…. And depending on the plant, (i.e.…
Health Law Is Reforming System Via Market Forces
All the controversial rhetoric about the new health reform law is missing a huge reality: The law is driving dramatic changes in the real world. Almost every major health delivery system is preparing to reorganize how they provide care to hundreds of millions of Americans by becoming Accountable Care Organizations (ACOs).
Health Systems are Voting With Their Wallets
The magnitude and level of financial interest in ACOs – and proof that it is not just cautious planning – were dramatically illuminated by recent actions and a Washington Post article:
- On Thursday, HHS released the long anticipated proposed rule for ACOs and Medicare “Shared Savings.”
Creating and Implementing Healthcare Innovation – BioPharmaceuticals, Delivery System and Reimbursements
Healthcare innovation is an extremely hot topic right now, ranging from the new Center for Medicare and Medicaid Innovation, FDA’s approach to approving therapies and devices, an entire issue of Health Affairs, and of course patient-centered medical homes and Accountable Care Organizations [Patient-centered medical homes are also known as Advanced Primary Care Model practices, and ACOs are a combination of delivery and reimbursement innovations.]
I’ve been working for many years to create value for patients and society by speeding adoption of these types of innovations by clinicians, other providers, patients, payers, regulators, communities, etc., and have found that healthcare innovations have at least three things in common:
- Healthcare innovations occur in steps, with each advance building on the shoulders of what came before
- These stepwise advances also produce indirect benefits that can be greater than the innovation’s direct effects
- Adoption of innovations doesn’t just “happen.”
Accountable Care Now
If all arrows in Washington pointed to the same spot for solving the healthcare and Federal spending problems could the politicians, pundits and policy people agree? Or would it take some new and powerful force to shine a spotlight and focus the collective vision on this solution, and what would that force be?
These are the two questions I’ve been asking myself as the battle over Federal spending has become near white-hot, and as it has become increasingly clearer that long-term Federal solvency and deficit reduction will require addressing the growth in healthcare spending – particularly Medicare.
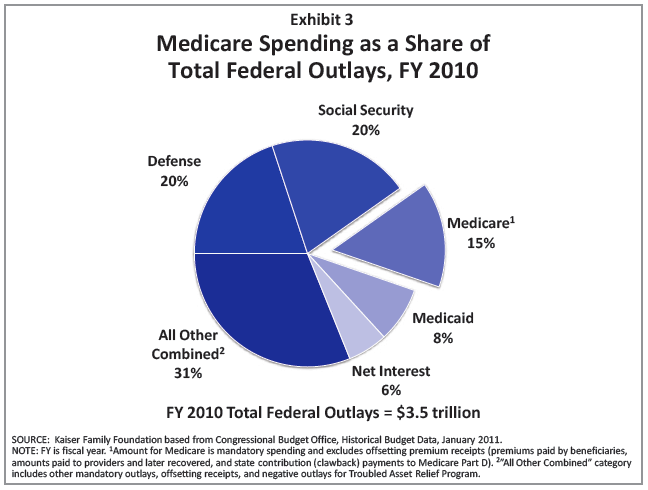 [Source: Kaiser Family Foundation “Medicare Spending and Financing,” February 2011]
[Source: Kaiser Family Foundation “Medicare Spending and Financing,” February 2011]
To summarize the highlights of this situation:
- Cutting non-defense discretionary Federal spending can’t produce the reductions needed to significantly impact the deficit – contrary to the general misunderstanding about how the Federal budget is spent.
Medical Homes (PCMH) in 2011 – Patient and Consumer Centric
Patient-Centered Medical Homes (PCMH) are continuing to be a bigger and broader part of the real-world discussions about health reform and transformation in the US. According to the the National Committee for Quality Assurance (NCQA) at the end of 2010 there were 7,676 clinicians in 1,506 recognized PCMH practices in the US. This information was released last week by NCQA with their updated 2011 PCMH Standards.
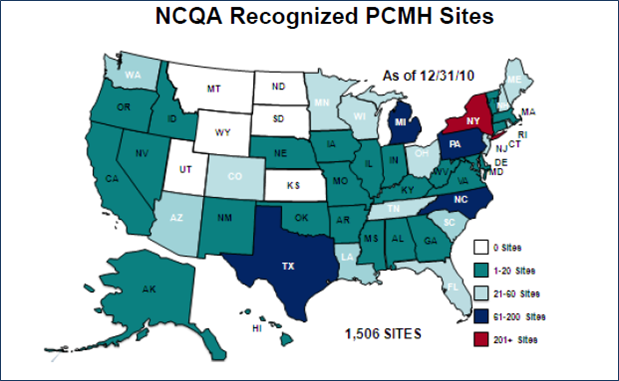
Another marker of medical homes’ increasing pervasiveness is the blurb – “Home sweet medical home” – in the March 2011 issue of Consumer Reports magazine that starts with, “If you haven’t already heard the term ‘patient-centered medical home,’ chances are you will soon.”…
Fundamentals of Health Reform and Transformation
Trying to follow what’s being written about implementing health reform has been like trying to drink a waterfall. Having followed these issues for many years I’ve gleaned some fundamental aspects about many of the ideas and recommendations that simplifies how to approach this flood – including how to evaluate ideas and proposals like Patient-Centered Medical Homes (PCMH), Accountable Care Organizations (ACO), Shared Savings, Health Information Exchanges (HIE), Pay-4-Performance (P4P), etc…
Structure v. Reimbursement Systems/Arrangements
First, discussions and descriptions that don’t affirmatively recognize the distinction between Structures and Reimbursement Systems can create significant confusion. For example, the requirements for a PCMH to be recognized by the National Commission for Quality Assurance are structural, but how they are reimbursed will strongly influence how successful such practices are for improving quality of care and controlling costs.…
US Healthcare Spending – 2009
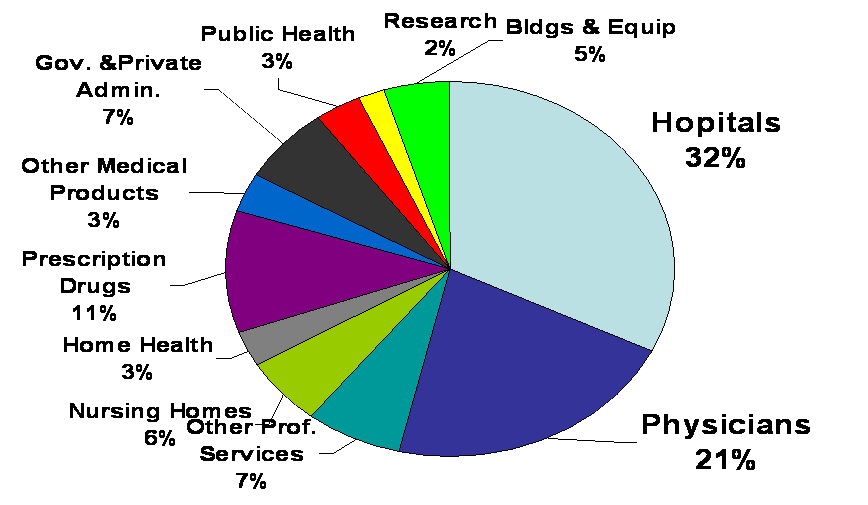
With all the focus on US health spending I thought it would be useful to update the pie chart I’d posted previously that showed 2007 and 2006 National Health Expenditures. So below is the chart showing US health spending for 2009.
{kind=link}
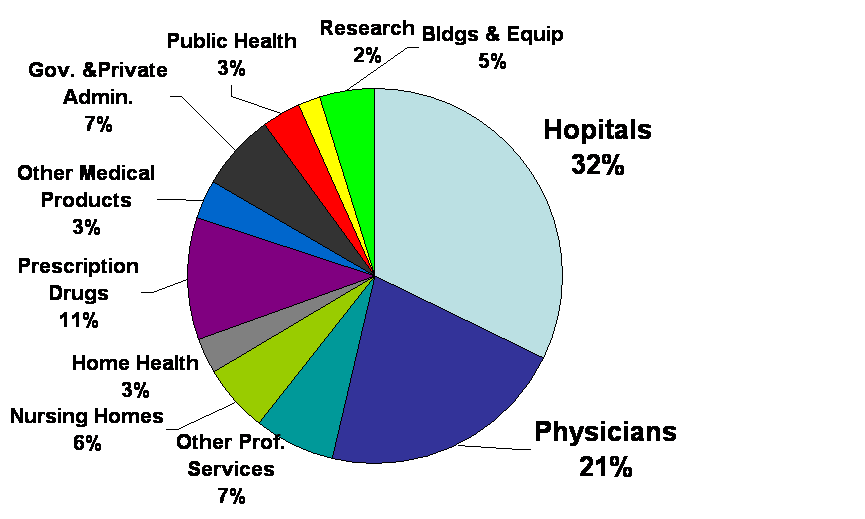
What can be seen by comparing this chart with the previous ones is that the percentages haven’t changed very much. Which means that the foci for cost containment still needs to be on hospitals and physician services and how they influence other types of spending. For example, avoiding hospital admissions, and utilizing clinical services provided by non-physician professionals, etc…. More on this to come in future posts.…