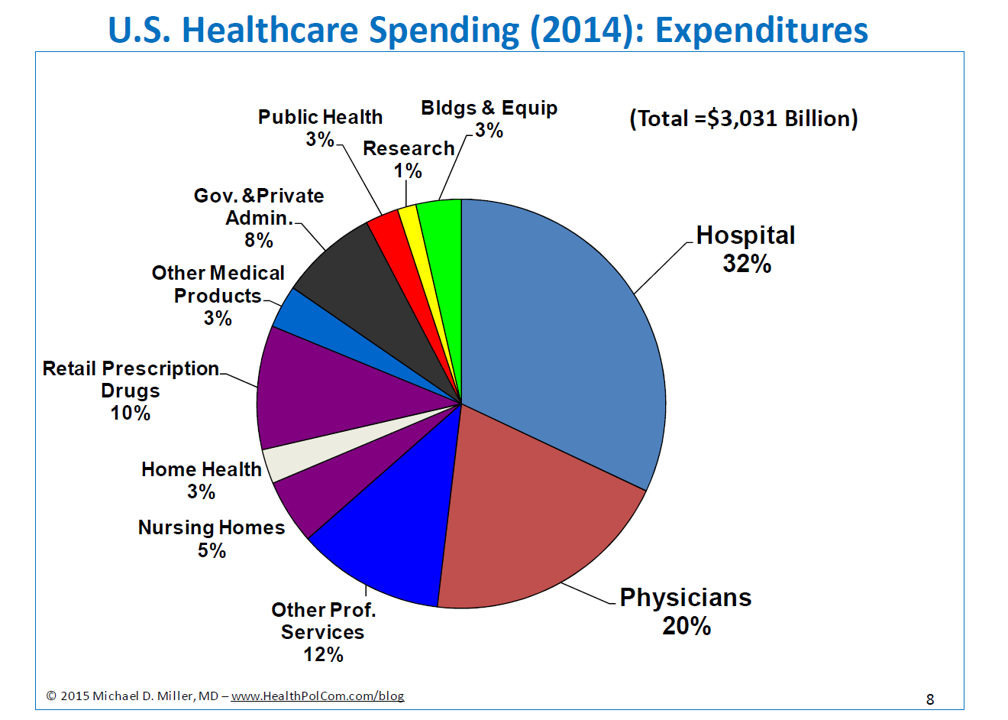
Why governments care about health spending and healthcare, how they are connected to overall government spending and priorities, and why addressing social determinants of health is so important for making lasting improvements, were the subjects I covered in a presentation at George Mason’s graduate policy school in September. My goal was to provide the soon-to-be policy analysts and advisers with a framework for understanding those issues so they will be able to provide useful recommendations to their future decision making bosses. (See the slide below for the topics covered in the presentation.) Links to videos of the talk are below, along with short descriptions – I think that Part 6 is particularly good.…
Health, Healthcare, and Government Spending (and a Culture of Health)